Gastrointestinální trakt a lymfatický systém
Enhancing lymphangiogenesis and lymphatic function
- Reduces experimental IBD
Adenoviral induction of prolymphangiogenic factor VEGF-C
- Provides marked protection against the development of acute and chronic colitis in 2 different animal models
VEGF-C-dependent protection
- Observed in combination with
- Increased inflammatory cell mobilization
- Bacterial antigen clearance from the inflamed colon to the draining lymph nodes
- VEGF-C/VEGFR3 pathway
- Regulates macrophage (Mfí) plasticity and activation
- In a STAT6-dependent manner
- Potential as a therapeutic strategy for IBD [53]
Blockade of PI3K signaling
- Acts downstream of activated VEG FR3
- Selectively afected the development of mesenteric, but not dermal, LVs (Stanczuk et al., 2015) [35]
Yersinia pseudotuberculosis infection in mice
- Even after mice recover from oral infection intestinal in?ammation continues
- Features reminiscent of Crohn’s disease
- Development of chronic in?ammation and impaired immunity
- Migratory DCs arising from the lamina propria failed to arrive in the draining lymph node
- Apparently because collecting vessels became excessively leaky
- Allowing for a spilling out of immune cells and chylomicrons within lymph into the adjacent fat [51]
Crohnova choroba
- Zánět zničí lymfatický zánět
- Kniha o lymfatickém systému u Crohnovy choroby (italský autor)
- Poškozený lymfatický systém se podílí některých obtížích
Crohn’s disease
- Creeping fat
- Expansion of fat in the mesentery
- Overrides the usual mesenteric border
- Extends up onto the intestinal wall [51]
- Collecting vessels are interrupted by the development of B cell–rich tertiary lymphoid structures
- Obstruct the path to the usual draining lymph node
- Tertiary lymphoid structures are common features in many inflammatory diseases and in cancers [51]
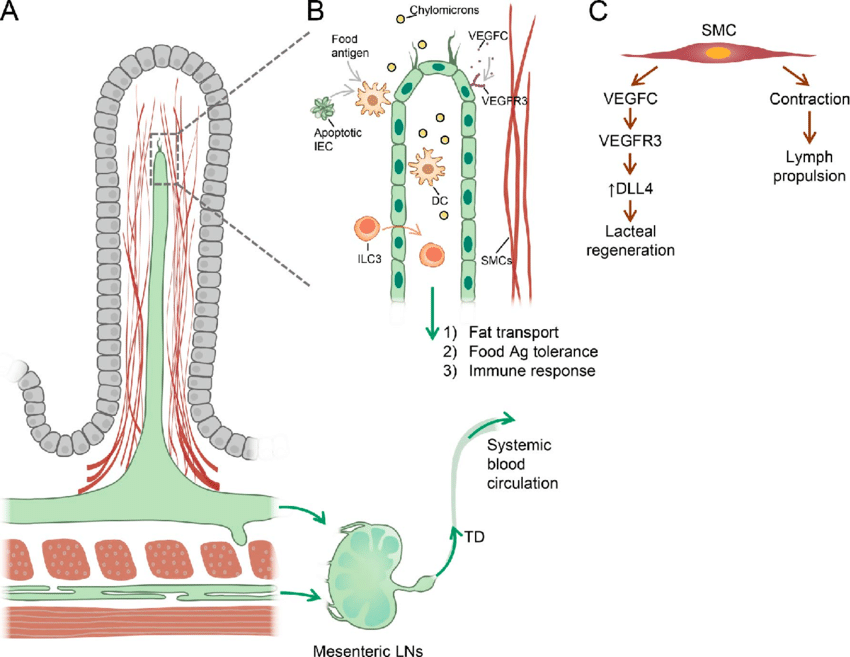
Lacteals
- Steady-state conditions and frequently harbor filopodia
- Ongoing lymphangiogenic response (Bernier- Latmani et al., 2015; Bernier-Latmani and Petrova, 2016) [35]
- Maintenance of lacteal integrity and fat transport function
- Requires continuous
- Notch
- VEGF-C–VEG FR-3 signaling
- VEGF-C being supplied by the surrounding smooth muscle cells (Bernier-Latmani et al., 2015; Nurmi et al., 2015) [35]
- Lacteals are characterized by mix of
- Continuous zipper junctions
- Discontinuous button-like junctions [35]
- Loss of Notch signaling
- Impairs the formation of mature button-like junctions (Bernier-Latmani et al., 2015) [35]
- Optimal junctional organization and transport function of lacteals
- Require
- Adrenomedullin-calcitonin receptor signaling [35]
- Lymphatic-specific inactivation of calcitonin receptor
- Results in intestinal lymphangiectasia and protein-losing enteropathy (Davis et al., 2017) [35]
- Intestine harbors a large population of immune cells
- Tune the balance between immune tolerance to the myriad of commensal intestinal bacteria and ingested harmless antigens [35]
- CCR7-expressing DCs migrate into intestinal lymphatics
- In response to the CCL21 gradient generated by LECs [35]
- Transport of food antigens by CD103+ DCs to mesenteric LNs
- Appears to be a key step in the establishment of oral tolerance
- Via induction of mesenteric LN T reg cells (Pabst and Mowat, 2012)
- Production T reg cells maintained by lymphatic traficking of DCs after ingestion of apoptotic intestinal epithelial cells
- Continuously produced as a result of rapid intestinal epithelium turnover (Cummings et al., 2016) [35]
- The CCR7+Rorgt+ subset of intestinal innate lymphoid cells
- Also egresses via intestinal LVs to mesenteric LNs [35]
- Pathological features of Crohn’s disease
- Increased lymphangiogenesis and lymphatic vascular dysfunction
- Lymphangiectasia
- Intralymphatic lymphocyte stasis (von der Weid et al., 2011) [35]
- Damage to lymphatic vasculatures and its unproductive expansion
- May be contributing / initiating factors in IBD (Bernier-Latmani and Petrova, 2017) [35]
- Diphtheria toxin–mediated conditional ablation of LVs in the intestine
- Leads to rapid animal demise
- Because of extreme disruption to the intestinal mucosal barrier and septic shock (Jang et al., 2013) [35]
Lymfovenosni anastomosa
- Co nejdříve po operacích se zásahem do uzlin
- Typicky v břiše po gynekologických operacích
- Lymforhoea x výtok po gynekologické operaci
- Leak do břišní dutiny
- Diskontinuita na LSG !!!
- Ideálně LSG co nejdříve po operaci se zásahem do uzlin
- Vždy doplnit lymfoscintigrafii po ukončení základní onkologické terapie
- Např. do 6 měs. po radioterapii
- Je vysoká pravděpodobnost vzniku lymfatické insufficience
- LSG hned po všech po OP
- Pokud bude diskontinuita na na LSG ke zvážení časné venoanastomosy !!!
- Doplnit i hluboký syst. LSG
Kam posílat
- Dr. Wald a Dr. Vlasák FN Motol
- Dr. Žernovický a Prof. Veselý z Brna
- Dr. Vidim - cévní chirurgie, primář v Kolíně
- Lymfo-venosní anastomosy v kubitě - jedný na světě
- Slovensko již také
- Prim. VFN Dr. Zámečník - OP lymfedem zadního genitálu a šourku
- Doc. Jarolím - výborný plast. chirurg urologie - op i lymfedemu
Leaking - high permeability of collecting vessels
- Vesseůs are known to have a basal level of permeability to proteins like albumin
- Permeability is suf?cient to broadcast antigens to DCs and macrophages that closely associate with the muscular wall of the collecting vessel
- Associated DCs appear to support collecting vessel integrity and lower permeability
- High permeability might be associated with infection or in?ammation-mediated loss or modi?cation of these support DCs [51]
Lymfatické cévy GIT
- Every villus contains a single blind-ended lymphatic capillary (lacteal)
- Underlying submucosa has its own lymphatic capillary network
- Muscularis too
- All independently intersect with, and drain into, contractile lymphatic collecting vessels [51]
- Originate at the mesenteric border
- Run antiparallel to the intestinal wall through mesenteric fat
- Until they reach mesenteric lymph nodes [51]
- In humans, there is a fourth lymphatic capillary bed that is located in the mesenteric fat itself
- Mostly localized just beneath the serosal epithelial covering of the mesenteric adipose tissue
- Four lymphatic capillary networks
- Carry many critical antigens to draining
- Lymph nodes, [51]
- Villus lacteals also transport dietary fat that is packaged into chylomicrons
- Mesenteric lymph node is subjected to periodic high loads of fat that ?lter through this space, [51]
- Has mechanisms to prevent fatty acid–driven in?ammation
- Microbial lipids are v.s. components of chylomicrons and regularly affect the mesenteric lymphatic corridor [51]
- Intestinal interstitial space and mesenteric lymphatic system provide a critical link between circulatory shock and the subsequent systemic inflammatory response syndrome
- www.frontiersin.org/articles/10.3389/fvets.2020.609583/full
Pankreatitida
- Nebiliárního původu začíná aseptickým edemem
- Až dodatečně se to ev. infikuje z GIT - sledováno na CT
- Pouze edem - chirurgický výkon ne (zinfikovalo by se to)
- Kdysi v Motole výkony lymfo-venosni anastomosy ductus thoracicus...
- Mesenteric lymphatic system allows proinflammatory agents to travel from the intestinal interstitial space to the general circulation bypassing the portal vein and liver. In 1970, Glenn and Lefer reported that diversion of thoracic duct lymph improved survival in a model of hemorrhagic shock (70). Later studies by Deitch et al. (71) focused on the intestinal interstitial space and its lymphatic drainage by demonstrating that while mesenteric lymph from a hemorrhagic shock model in rats was cytotoxic, portal vein plasma was not (71–73). In addition, when mesenteric lymph is prevented from entering the circulation, shock-induced injury to lung and heart is avoided and survival is enhanced (71, 74). Models of intestinal ischemia/reperfusion rather than hypovolemic shock showed similar results. Mesenteric lymph collected following intestinal hypoperfusion and, then, administered intravenously to clinically normal animals provokes tissue injury affecting the lungs and heart (75–77). Similarly, the myocardial edema induced in a canine model of mesenteric ischemia/reperfusion is eliminated by diversion of mesenteric lymph (75).
Vagal nerve stimulation also increases intestinal blood flow, prevents intestinal barrier dysfunction, markedly decreases lung inflammation and inhibits development of inflammatory and cytotoxic activity in mesenteric lymph subsequent to hemorrhagic shock (82–86). As a therapeutic modality, vagal nerve stimulation is currently impractical. However, a pharmacologic vagal agonist, CPSI-121, also prevents intestinal injury and acute lung injury as well as attenuates development of inflammatory activity in mesenteric lymph following induction of hemorrhagic shockcytotoxic element in the affected mesenteric lymph has been addressed by several investigations focused on the entry of bacteria and endotoxin from the GI tract and activation of endogenous proinflammatory mediators (68). The hypothesis with the strongest current evidentiary support involves passage of pancreatic digestive enzymes through a damaged intestinal mucosa into the interstitial space. Mitsuoka et al. (89) demonstrated that luminal dilution and inhibition of digestive pancreatic enzymes diminished the lung injury induced by intestinal ischemia/reperfusion. Subsequently, they and others have provided evidence that intestinal hypoperfusion and ischemia/reperfusion injury lead to mucosal barrier disruption and entry of luminal components including free fatty acids and digestive enzymes from the exocrine pancreas into the intestinal interstitium (90–92). Once there, the pancreatic enzymes begin to digest interstitial components to produce novel inflammatory and cytotoxic agents such as unbound free fatty acids (93). These pancreatic enzymes and cytotoxic agents can then gain access to the general circulation via the mesenteric lymphatics as well as by the portal circulation and peritoneal cavity (71, 74, 94). Interruption of this pathologic cascade leads to more positive outcomes. Intraluminal administration of a protease inhibitor and a gastric and pancreatic lipase inhibitor reduces intestinal tissue injury and improves cardiovascular function (95). In addition, blockade of pancreatic enzymes within the bowel lumen increases survival in three forms of experimental shock caused by hemorrhage, septic peritonitis and intravenous endotoxin (96). Three different protease inhibitors instilled directly into the small intestine 1 h after initiation of the shock episode were all shown to have a beneficial effect (96).https://www.frontiersin.org/articles/10.3389/fvets.2020.609583/full
Slinivka
- Před cca 20 lety
- U aktuní pankreatitidy se rozšiřoval ductus thoracicus
- První zánět - mnoho prozánětlivých cytokinů a proteolytických enzymů
- Když není drenáž do cév, hrozí rozpad slinivky
- Zvažovala se porucha drenáže retroperitoneálního prostoru